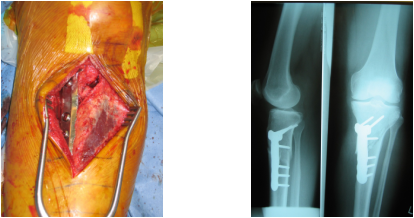
The BURN upper tibial osteotomy with tricortical autologous bone grafting is a simple and reliable method to correct the varus knee. The tibial tubercle is not moved laterally as it is with a Pudu supra-tubercle osteotomy. The bone is cut from anterior to posterior so avoiding posterior venous damage and DVT causation. The lateral cortex is NOT cut and finishes in the cancellous bone at a 3.2 mm drill hole. The osteotomy is wedged open with a Bristow by gentle rotation.
This osteotomy has been done concurrently with a medial Oxford UNI, where there is significant tibia vara. The tibial cutting jig of the UNI is lined up to a virtual correction point, which is lateral to the normal aiming point. The tibia will be corrected to this point with the opening of the osteotomy. The hemi knee is done balancing the soft tissues, as the final alignment will be adjusted by the osteotomy. Graft form the hemi goes into the osteotomy.
DO NOT USE BONE GRAFT SUBSTITUTES AS PUBLISHED BY HOOPER, SCHOUTEN et al.
In my hands there have been no cases of DVT in contrast to the lateral closing wedge osteotomy which in my hands has the highest risk of DVT of all lower limb operations. The UTMOWO is easy to convert to TKR, with results the same as primary TKR (compare with lateral closing wedge (COVENTRY STYLE) converted, which is equivalent to a revision knee) Make sure the patient is off all NSAIDS 7 days before surgery and until union and is a non-smoker.
This osteotomy has been done concurrently with a medial Oxford UNI, where there is significant tibia vara. The tibial cutting jig of the UNI is lined up to a virtual correction point, which is lateral to the normal aiming point. The tibia will be corrected to this point with the opening of the osteotomy. The hemi knee is done balancing the soft tissues, as the final alignment will be adjusted by the osteotomy. Graft form the hemi goes into the osteotomy.
DO NOT USE BONE GRAFT SUBSTITUTES AS PUBLISHED BY HOOPER, SCHOUTEN et al.
In my hands there have been no cases of DVT in contrast to the lateral closing wedge osteotomy which in my hands has the highest risk of DVT of all lower limb operations. The UTMOWO is easy to convert to TKR, with results the same as primary TKR (compare with lateral closing wedge (COVENTRY STYLE) converted, which is equivalent to a revision knee) Make sure the patient is off all NSAIDS 7 days before surgery and until union and is a non-smoker.
