Planning is essential for consistent outcomes
|
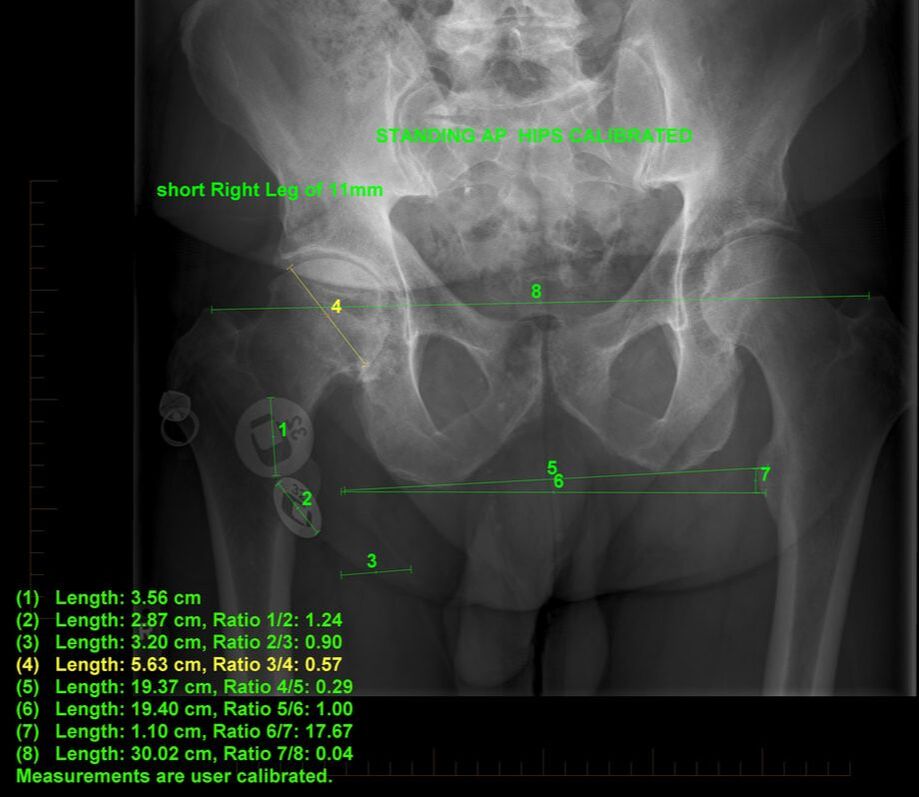
Radiology needs to be complete with standing calibrated AP radiographs, a Standing Direct Lateral with the hip of interest away from the "film" ( knees slightly flexed if there is a Fixed flexion deformity of the hips), and an orthogonal shoot-through lateral image with standardised radiographic techniques. Templating systems must be available. I use equal size calibration marker discs (32mm) on the anterior and posterior aspect of the hip at the time of standing AP X-rays. [(D1-D2)/2 + D2]/32 = magnification. A simpler way is to draw a line on the computer image of length (D1 + D2)/2 and then set this line's length as 32mm. Now adjust the image size, so that the ruler on the screen matches your template's ruler. Now you are done! (A MARKER OF A KNOWN SIZE IN THE MIDAXIAL PLANE IS EXCELLENT BUT "INVASIVE" ) TraumaCad (commercial software from Brainlab) still requires calibration and is complicated for nurse to use intra-operatively if needed. |
|
|

|
Surgeons need to be familiar with several different hip systems to cope with differing anatomy and bone quality and be aware of the track record of these devices.
FIXATION
In my practice, cemented acetabular components for primary THR would be less than 1%. They simply are not needed. One of my currently used cups (Mathys Vitamys press-fit) provides an excellent alternative incorporating Vit E stabilised Polyethylene, but over-ream by 1mm. Beware of your reamers, many are atrociously engineered being non-spherical and overly aggressive "bite" to the teeth can result in oval reaming!
In younger active patients the LIMA PF SHELL with Delta Ceramic a Ceramic on Ceramic is used. It has a long taper to lock the ceramic liner and a user-friendly impactor.
In younger active patients the LIMA PF SHELL with Delta Ceramic a Ceramic on Ceramic is used. It has a long taper to lock the ceramic liner and a user-friendly impactor.
BEARING COUPLINGS
HARD ON SOFT OPTIONS
The issue of plastic wear (polyethylene, PE) be that standard or highly cross-linked is a concern. There are good manufacturers with proven devices and there have been some very poor ones! Vitamin E Polyethylenes appear to improve wear characteristics but "cold flow" from edge-loading in mal-positioned cups is still a major issue that will likely result in late dislocations.
Sulzer (now Zimmer), Mathys, Smith and Nephew and Biomet to name a few, have been very good in my experience. It comes down to their suppliers of 1020 or 1050 resins and how the plastic is treated and sterilised by the manufacturer though.
The early Duroloc cup liners sterilised in air, Hylamer, a highly cross-linked and more crystalline PE, and Gas plasma sterilized Enduron have performed badly in NZ. Failure has occurred within 4 years in some cases, with excess wear and osteolysis and sub-surface oxidation.
I have experience of failed Oxinium on PE from Smith and Nephew, a case revised from another centre, where several dislocations had scratched the head severely and caused rapid wear of the polyethylene liner. The heads are not as resilient as a Delta ceramic head to damage though.
The issue of plastic wear (polyethylene, PE) be that standard or highly cross-linked is a concern. There are good manufacturers with proven devices and there have been some very poor ones! Vitamin E Polyethylenes appear to improve wear characteristics but "cold flow" from edge-loading in mal-positioned cups is still a major issue that will likely result in late dislocations.
Sulzer (now Zimmer), Mathys, Smith and Nephew and Biomet to name a few, have been very good in my experience. It comes down to their suppliers of 1020 or 1050 resins and how the plastic is treated and sterilised by the manufacturer though.
The early Duroloc cup liners sterilised in air, Hylamer, a highly cross-linked and more crystalline PE, and Gas plasma sterilized Enduron have performed badly in NZ. Failure has occurred within 4 years in some cases, with excess wear and osteolysis and sub-surface oxidation.
I have experience of failed Oxinium on PE from Smith and Nephew, a case revised from another centre, where several dislocations had scratched the head severely and caused rapid wear of the polyethylene liner. The heads are not as resilient as a Delta ceramic head to damage though.
HARD ON HARD OPTIONS
Metal on Metal (MoM):
Advantage is no fracturing or squeaking.
Disadvantage is metal ion toxicity and potential oncologic effects.
Not all are equal in alloys and manufacture. For example, even the materials can be identical but the geometry different.
Metal on Metal (MoM):
Advantage is no fracturing or squeaking.
Disadvantage is metal ion toxicity and potential oncologic effects.
Not all are equal in alloys and manufacture. For example, even the materials can be identical but the geometry different.
|
EXCELLENT: METASUL - Fitmore (in both 28mm and 32mm) with no cases of ALVAL (Aseptic Lymphocyte-dominated Vasculitis Associated Lesion) in my cases. Risk of neck impingement high in 28mm articulations.
Follow up of >21 years in young males of 130kg, normal radiographs and normal plasma metal ion levels... (have we thrown the baby out with the bath water!!??) POOR: The Artek cup, a shallow "dysplastic" acetabular cup is no longer made. It was made of the same alloy as Metasul and demonstrates many engineering design faults. ASR recalled (J&J), Durom withdrawn, Surface replacements now doing badly, along with large ball MoM conventional THR. The latter due to taper junction loosening (cause poor design and engineering ?510K validation inappropriate - author's opinion) |
Ceramic on Ceramic (CoC):
Biolox Forte / Delta (Ceramtec)
Advantage is no metal ion toxicity and wear is minimal.
Disadvantage is potential fracture and squeaking ?due to mal-placement, poor seating or chipping at time of insertion and even "distortion" of the shell and liner during impaction. (It is more difficult to engineer a Hard on Hard Hip Bearing than a "non-congruent" total knee replacement which uses a soft bearing material.)
Biolox Forte / Delta (Ceramtec)
Advantage is no metal ion toxicity and wear is minimal.
Disadvantage is potential fracture and squeaking ?due to mal-placement, poor seating or chipping at time of insertion and even "distortion" of the shell and liner during impaction. (It is more difficult to engineer a Hard on Hard Hip Bearing than a "non-congruent" total knee replacement which uses a soft bearing material.)
|
EXCELLENT: Delta on Delta - better than Forte and excellent to date but need careful follow-up.
VERY GOOD: Biolox Forte on Biolox Forte (Ceramtec, Germany. One fracture of a Forte liner (Refection, S&N) from trauma. No fractures with Biolox Delta. This is no longer an acceptable coupling. POOR: Zirconia heads from Saint-Gobain running on PE. These heads have been withdrawn and grain drop-out may have been the cause, including a new tunnel manufacturing process. Bionit on Bionit are failing now (2016) and Ceramys on Ceramys (Mathys, Switzerland) are no longer available (as of 2015). |
NOVEL BEARING COUPLINGS
Ceramic on Metal:
I have one case at 7 years. Although totally asymptomatic with no squeaking or osteolysis, there is high metal ion level in the joint fluid (> 5000nmol/L of Cr!) which is not seen in peripheral blood. Beware! I would avoid this combination. There is no advantage over MoM and Co and Cr levels in the hair are high in MoM.
Ceramic on Polyimide:
This is a high performance bearing material used in jet engines. I have 1 case now at 17 years and the other died at 6.5 years (the first patients in the world). The 17yr case is asymptomatic and no change or radiographic evidence of wear and osteolysis. This material has proven itself to be as good as the best to date.
Ethical Committee approval was gained to do a cohort of 100 patients which started in October 2012, and now there are 100 patients in the cohort with 6 revisions. These revisions were for stem issues in 3 cases with the HA coming off the Evolutis Stemsys cementless stems. There were 3 cases where the clearance between the head and the liner was too tight. These liners locked into the "Ceramtec" taper. There was no osteolysis and a simple exchange to a PE liner was done. Disappointing but easily corrected with appropriate engineering and testing!!
Wear was less than 1 micron per year in a post-mortem case at 6.5 years. This material does not wear or "cold flow" like Polyethylenes, so engineering has to be more rigorous.
Results presented COMOC 2016 and latest results at ISTA HAWAII 2022. (This is an exciting material and when "picked up" by a large player, will change orthopaedics due to its remarkable properties and biocompatibility.)
Hard on Soft:
There is hard on very soft polycarbonate/polyurethane, again new and I have no personal experience of this. In Australia there are some 3.5 year results. We await their publication of these (see JRI for details).
Silicon Nitride on Silicon Nitride:
A new couple currently being trialled in South Africa. This is hoped to outperform "Delta" ceramic from Ceramtec, being tougher and more chip-resistant.
Ceramic on Metal:
I have one case at 7 years. Although totally asymptomatic with no squeaking or osteolysis, there is high metal ion level in the joint fluid (> 5000nmol/L of Cr!) which is not seen in peripheral blood. Beware! I would avoid this combination. There is no advantage over MoM and Co and Cr levels in the hair are high in MoM.
Ceramic on Polyimide:
This is a high performance bearing material used in jet engines. I have 1 case now at 17 years and the other died at 6.5 years (the first patients in the world). The 17yr case is asymptomatic and no change or radiographic evidence of wear and osteolysis. This material has proven itself to be as good as the best to date.
Ethical Committee approval was gained to do a cohort of 100 patients which started in October 2012, and now there are 100 patients in the cohort with 6 revisions. These revisions were for stem issues in 3 cases with the HA coming off the Evolutis Stemsys cementless stems. There were 3 cases where the clearance between the head and the liner was too tight. These liners locked into the "Ceramtec" taper. There was no osteolysis and a simple exchange to a PE liner was done. Disappointing but easily corrected with appropriate engineering and testing!!
Wear was less than 1 micron per year in a post-mortem case at 6.5 years. This material does not wear or "cold flow" like Polyethylenes, so engineering has to be more rigorous.
Results presented COMOC 2016 and latest results at ISTA HAWAII 2022. (This is an exciting material and when "picked up" by a large player, will change orthopaedics due to its remarkable properties and biocompatibility.)
Hard on Soft:
There is hard on very soft polycarbonate/polyurethane, again new and I have no personal experience of this. In Australia there are some 3.5 year results. We await their publication of these (see JRI for details).
Silicon Nitride on Silicon Nitride:
A new couple currently being trialled in South Africa. This is hoped to outperform "Delta" ceramic from Ceramtec, being tougher and more chip-resistant.
HEAD SIZE AND ACETABULAR SHAPE
The larger the head:neck ratio, the greater the stability. But the acetabular component must not be dysplastic (<180 degrees) or edge loading and "stripe wear" will occur. The mistake most manufacturers have made, is that they have made "dysplastic components" (ASR, DUROM, ARTEK). Heads >36mm increase the risk of taper loosening if there is edge loading resulting in increasing friction and therefore torque on the trunnion.
Long-term results with large heads on PE are not available yet and caution should be exercised, due to thin PE and surgeons removing more native bone chasing "stability".
BIPOLAR designs use large "internal" heads of Polyethylene on COCr acetabular components with a smaller ceramic or metal head within the polyethylene. There is merit in this design which is more forgiving with regard to "neck on cup" impingement and stability and useful in revision procedures for dislocations. ( Note: If there has been ceramic or metal debris then this gets imbedded in the outer surface of the large PE head and will cause marked metal wear!)
"Golf ball" type surface modification on heads for hard on soft couplings may prove helpful in reducing friction through boundary lubrication effects.
Long-term results with large heads on PE are not available yet and caution should be exercised, due to thin PE and surgeons removing more native bone chasing "stability".
BIPOLAR designs use large "internal" heads of Polyethylene on COCr acetabular components with a smaller ceramic or metal head within the polyethylene. There is merit in this design which is more forgiving with regard to "neck on cup" impingement and stability and useful in revision procedures for dislocations. ( Note: If there has been ceramic or metal debris then this gets imbedded in the outer surface of the large PE head and will cause marked metal wear!)
"Golf ball" type surface modification on heads for hard on soft couplings may prove helpful in reducing friction through boundary lubrication effects.
FEMORAL STEM
NECK-SHAFT ANGLE:
Beware the low FEMORAL neck-shaft angle as this promotes taper looseningand impingement in abduction of correctly placed acetabular components.
FEMORAL VERSION:
For "human bipedal gait" as opposed to quadrupeds, make sure the version (or more correctly, anterior "offset displacement") is correct. If you are using a non-anatomical stem, then the posterior entry to the canal will require a greater than "normal" anteversion. Typical version is 20 degrees. This is a very common mistake made and overlooked in almost all studies. The pro-op standing direct lateral film is most useful and to compare with the post-op same radiograph.
Beware the low FEMORAL neck-shaft angle as this promotes taper looseningand impingement in abduction of correctly placed acetabular components.
FEMORAL VERSION:
For "human bipedal gait" as opposed to quadrupeds, make sure the version (or more correctly, anterior "offset displacement") is correct. If you are using a non-anatomical stem, then the posterior entry to the canal will require a greater than "normal" anteversion. Typical version is 20 degrees. This is a very common mistake made and overlooked in almost all studies. The pro-op standing direct lateral film is most useful and to compare with the post-op same radiograph.
ACETABULAR PLACEMENT
Correct opening is 35 to 40 degrees inclination from the horizontal on a Standing AP radiograph and anteversion 25 to 30 degrees on a Standing direct lateral radiograph. Those with a stiff spine should have a sitting Direct Lateral Radiograph pre-operativel also for planning correct ante-version. This is patient specific and promotes stability and lubrication.
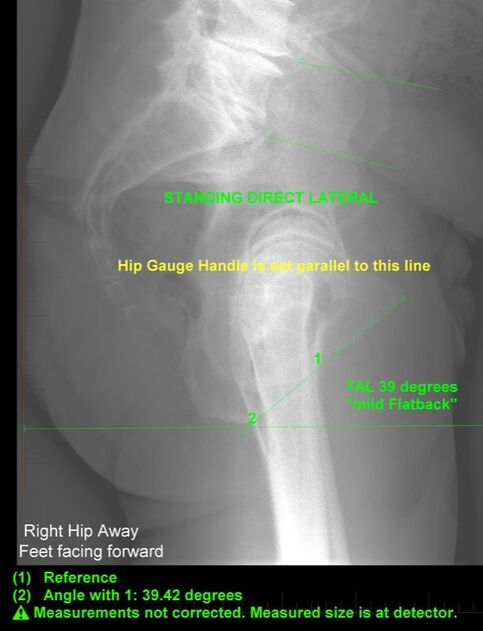
Getting this correct is very important. Use of BURN's line - a projection of a line drawn on the patient from the underside of the symphysis pubis to the inferior aspect of the ischium (gluteal crease) - facilitates this. This line is drawn on the Standing Direct Lateral Radiograph visible at all times during the precedure. The Hip Calibration Gauge handle is set parallel to BURN's line before making the skin incision, (Check with the fingers through the drape the ischial line and true position as sticky drapes can pull the posterior skin a little!). When components are correct, then at the combined 20/20 flexion/internal rotation, the head and acetabulum will be totally concentric, provided the neck shaft angle is 135 degrees. (If a more valgus stem is chosen then the cup will appear more open and vice versa).
In general, with the cup placed at 90 degrees to this line will give the correct anteversion in most cases but... correct acetabular placement can be verified by a direct standing and sitting lateral done pre-operatively. Beware the "FLATBACK SYNDROME" before THR.
Getting this correct is very important. Use of BURN's line - a projection of a line drawn on the patient from the underside of the symphysis pubis to the inferior aspect of the ischium (gluteal crease) - facilitates this. This line is drawn on the Standing Direct Lateral Radiograph visible at all times during the precedure. The Hip Calibration Gauge handle is set parallel to BURN's line before making the skin incision, (Check with the fingers through the drape the ischial line and true position as sticky drapes can pull the posterior skin a little!). When components are correct, then at the combined 20/20 flexion/internal rotation, the head and acetabulum will be totally concentric, provided the neck shaft angle is 135 degrees. (If a more valgus stem is chosen then the cup will appear more open and vice versa).
In general, with the cup placed at 90 degrees to this line will give the correct anteversion in most cases but... correct acetabular placement can be verified by a direct standing and sitting lateral done pre-operatively. Beware the "FLATBACK SYNDROME" before THR.
HIP CAPSULE REPAIR
The hip capsule must be repaired as it is this structure that stops dislocation and redirects the joint reaction force. (In >1600 consecutive posterior approach primary THR's, no dislocations (author).
CURRENT RESEARCH AND AUDIT
I have 40 patients who have bilateral THR's, one CoC and the other MoM (Metasul) articulations. There is no difference clinically, but the bone at the neck resection seems to grow back up the neck slightly in the CoC cases, which may indicate a more bone friendly environment.
I have no cases of my own of Pseudotumour in MoM, even with the Biomet system previously available of which I did about 10 cases. We have resected a pseudotumour in a ceramic on polyethylene done 6 years ago. This was due to a loose ceramic head on a cobalt chrome AML stem. Paprosky et al have published on metal ions released from tapers and this may be the primary site of release. Chromium slats released from corrosion are more toxic and of higher valency than those from mechanical fretting.
Currently I am the only surgeon in New Zealand using Polyimide in THR and following these patients very closely. The results are looking excellent with patients playing squash, skiing, mountain running and biking! The material is being given a very good "workout"!
NOTE; In New Zealand all our patients are registered on the NZJR, and independent audit of our cases is undertaken continuously.
I have no cases of my own of Pseudotumour in MoM, even with the Biomet system previously available of which I did about 10 cases. We have resected a pseudotumour in a ceramic on polyethylene done 6 years ago. This was due to a loose ceramic head on a cobalt chrome AML stem. Paprosky et al have published on metal ions released from tapers and this may be the primary site of release. Chromium slats released from corrosion are more toxic and of higher valency than those from mechanical fretting.
Currently I am the only surgeon in New Zealand using Polyimide in THR and following these patients very closely. The results are looking excellent with patients playing squash, skiing, mountain running and biking! The material is being given a very good "workout"!
NOTE; In New Zealand all our patients are registered on the NZJR, and independent audit of our cases is undertaken continuously.
